The Problem
Anterior knee pain is one of the most common (up to 40%) complaint from patients, active or sedentary who are attending a sports injury clinic.
Patellofemoral pain is defined as pain in front of the knee, around or behind the knee cap (patella) usually aggravated by activities that load the patellofemoral joint such as ascending or descending stairs, jumping, running and squatting (Crossley et al., 2016)
Most young patients have no structural damage to their patellofemoral joint and their symptoms are caused by a functional imbalance. Some patients have structural changes such as chondral and osteochondral degenerative changes and some patients suffer with overuse injuries of the extensor mechanism (tendonitis and insertional tendinosis) or patella instability (Petersen et al, 2014).
Older patients usually present with established patellofemoral osteoarthritis.
Despite the high prevalence of patellofemoral pain there are few published guidelines to help clinicians recommending an evidence based treatment for their patients.
The Cause
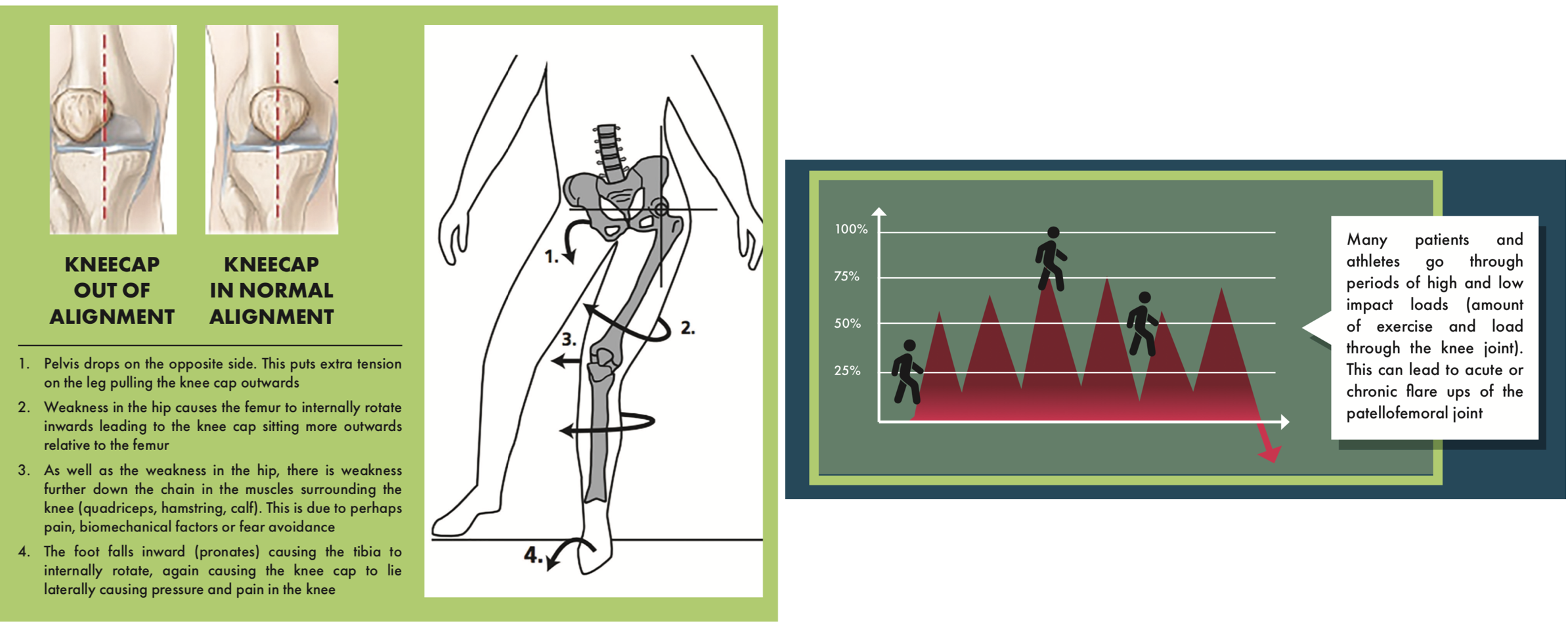
It is unsure as to exactly the reason why patients have patellofemoral pain but the latest scientific research indicate towards contributing factors being patella maltracking, dynamic valgus, muscular dysfunction, foot disorders and psychological factors (Petersen et al, 2014).
The Treatment
The consensus statement from the 4th International Patellofemoral Pain Research Retreat in 2016 include four main treatment recommendations.
1. Exercise-therapy is recommended to reduce pain in the short, medium and long term, and improve function in the medium and long term.
2. Combining hip and knee exercises is recommended to reduce pain and improve function in the short, medium and long term, and this combination should be used in preference to knee exercises alone.
3. Combined interventions are recommended to reduce pain in adults with patellofemoral pain in the short and medium term.
4. Foot orthoses are recommended to reduce pain in the short term.
Many studies have found that Exercise-therapy is the key component to patellofemoral rehabilitation. A robust body of evidence (60 high & moderate quality published papers and systematic reviews including meta-analysis) reports significant pain reduction and improvement in function with Exercise-therapy compared to control, placebo interventions in the short and medium time to follow up. The existing evidence also highlights the importance of long term management for these patients.
Combined interventions included exercise therapy, patellar taping, patellar mobilisations and prescription of foot orthoses. This approach was found to reduce pain in the short and medium term and reduce pain among adolescents in the longer term (Barton et al., 2015)
This evidence underpins the approach we take in our clinic towards the patients with anterior knee pain and patellofemoral pathology and the treatment we recommend those patients.
We offer our patients a multimodal approach to rehabilitating patellofemoral pain in order to reduce pain and improve function in the short, medium and long term.
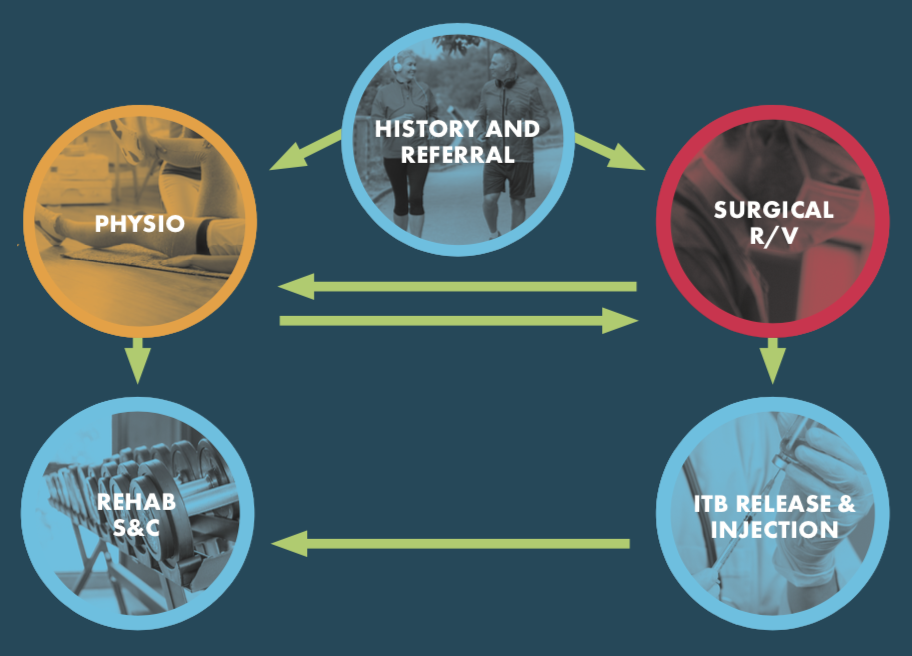
The Patellofemoral Pain Pathway
Our aims are to firstly diagnose and educate our patients.
Knowledge is power regarding patellofemoral pain and we understand that patient education is a key component to ensure compliance, avoid overloading and attain a quick referral for further intervention if and when required.
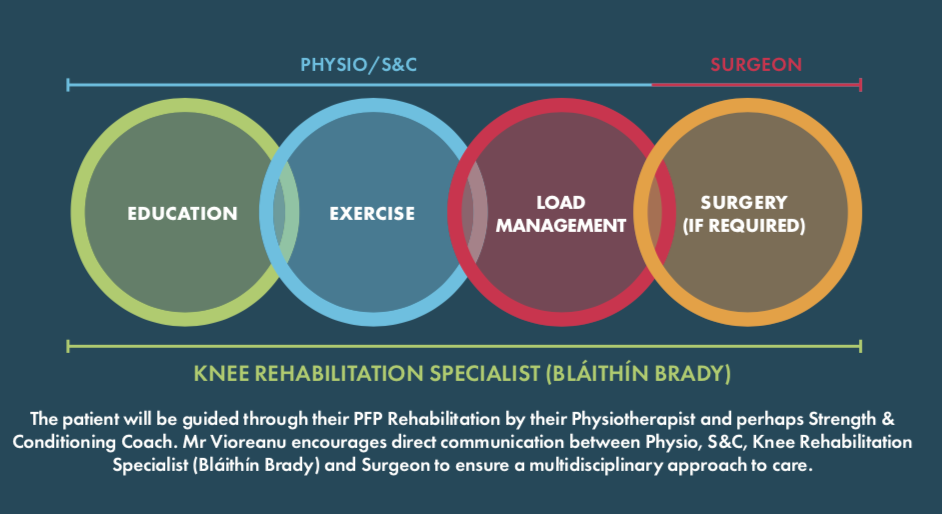
As a knee surgeon and as a specialist knee physiotherapist, we understand that patellofemoral pain is difficult to treat. We emphasise that regular, specific exercise and in particular following a specific strength & conditioning program is the most common treatment for patellofemoral pain.
Patients with more severe presentation and who are resistant to conservative measures often need anti-inflammatory medication, and in some cases an intra-articular injection.
For patients who are not improving their symptoms despite a rigorous conservative treatment as described above, Mr. Vioreanu recommends a surgical procedure called an iliotibial band (ITB) release. The ITB release is a simple, minimally invasive and effective day case surgical procedure that through a small (less than 2 cm) incision lengthens the iliotibial band and as a consequence releases the pressure from the patellofemoral joint.
The surgery along with the recommended immediate postoperative rehabilitation program provides a window of opportunity for patients to engage in the further more structured rehabilitation in order to return to their desired level of activities.
You can download here our Patellofemoral Pain Rehabilitation Protocol
References:
- Barton CJ, Crossley KM. Sharing decision-making between patient and clinician: the next step in evidence-based practice for patellofemoral pain? Br J Sports Med 2016;50:833–4
- Barton CJ, Lack S, Hemmings S, et al. The ‘Best practice guide to conservative management of patellofemoral pain’: incorporating level 1 evidence with expert clinical reasoning. Br J Sports Med 2015;49:923–34
- Crossley KM, Dorn TW, Ozturk H, van den Noort J, Schache AG, Pandy MG. Altered hip muscle forces during gait in people with patellofemoral osteoarthritis. Osteoarthritis Cartilage. 2012;20(11):1243–1249.
- Crossley KM, Stefanik JJ, Selfe J, et al. Patellofemoral pain consensus statement
from the 4th international patellofemoral pain research retreat, Manchester. part 1 terminology, definitions, clinical examination, natural history. Br J Sports Med 2016;2016:839–43. - Crossley KM, van Middelkoop M, Callaghan MJ, Collins NJ, Rathleff MS, Barton CJ. 2016 Patellofemoral pain consensus statement from the 4th International Patellofemoral Pain Research Retreat, Manchester: part 2. Recommended physical interventions (exercise, taping, bracing, foot orthoses and combined interven- tions). Br J Sports Med. 2016;50(14):844–852.
- Esculier JF, Bouyer LJ, Dubois B, et al. Is combining gait retraining or an exercise programme with education better than education alone in treating runners with patellofemoral pain? a randomised clinical trial. Br J Sports Med 2017:bjsports-2016-096988 (Epub ahead of print)
- Lack S, Barton C, Sohan O, et al. Proximal Muscle Rehabilitation is effective for patellofemoral pain: a systematic review with meta-analysis. Br J Sports Med 2015;49:1365–76
- Lack S, Barton C, Vicenzino B, et al. Outcome predictors for conservative patellofemoral pain management: a systematic review and meta analysis. Sports Med 2014;44:1703–16.
- Peters JS, Tyson NL. Proximal exercises are effective in treating patellofemoral pain syndrome: a systematic review. Int J Sports Phys Ther 2013;8:689–700
- Petersen W, Ellermann A, Gösele-Koppenburg A, et al. Patellofemoral pain syndrome. Knee Surg Sports Traumatol Arthrosc. 2014;22(10): 2264–2274.
- Rathleff MS, Roos EM, Olesen JL, et al. Exercise during school hours when added
to patient education improves outcome for 2 years in adolescent patellofemoral 51 pain: a cluster randomised trial. Br J Sports Med 2015;49:406–12 - Selfe J, Callaghan M, Witvrouw E, et al. Targeted interventions for patellofemoral pain syndrome (TIPPS): classification of clinical subgroups. BMJ Open. 2013;3(9):e003795
- Thomas MJ, Wood L, Selfe J, Peat G. Anterior knee pain in younger adults as a precursor to subsequent patellofemoral osteoarthritis: a systematic review. BMC Musculoskelet Disord. 2010;11:201–210.
- van der Heijden RA, de Kanter JL, Bierma-Zeinstra SM, et al. Struc- tural abnormalities on magnetic resonance imaging in patients with patellofemoral pain: a cross-sectional case-control study. Am J Sports Med. 2016;44(9):2339–2346.